
|
||||||
|---|---|---|---|---|---|---|
| Echocardiography 5 minutes before starting
|
||||||
Cardiac function and PA pressure |
||||||
|
—Echocardiographic examinations |
—Cardiac function and PA pressure |
—Examples of pathological |
||||
| Longitudinal ventricular function | ||||||
|
|
||||||
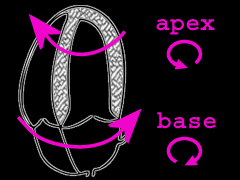
Leonardo da Vinci described as early as 1478, that contracting hearts showed a movement from the base to the apex
during each cardiac systole. Ventricular torsion was first described by William Harvey in 1628. Recently, a new
dissection technique developed by
Francisco Torrent Guasp
and published in 1980, could show the complexity of myocardial architecture, explaining all types of
cardiac movement during the heart function.
Quantitative assessment of longitudinal venticular function |
||||||
|
|
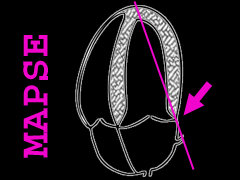
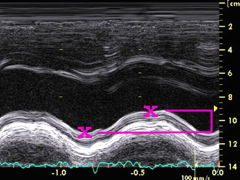
Left:
MAPSE is assessed with M-mode in apical four-chamber view, placing the examination beam on the lateral
mitral annulus. |
||||
|
|
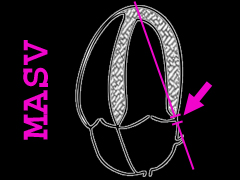
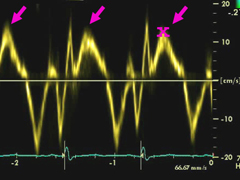
Left:
pulsed TDI sample volume is placed on the lateral mitral annulus to assess systolic velocities.
Possible oscillation due to respiration, as well as by MAPSE, should also be avoided here. |
||||
|
2D Speckle-Tracking Strain The longitudinnal strain in this case is normal. In this case, the longitudinal strain is mildly reduced, especially septal basal. Here is an example of a moderate reduction of the longitudinal strain, especially mediobasal, in a case of cardiac compromise by systemic light-chain amyloidosis. The apical segments show normal values (relative apical sparing). The longitudinal strain is in this case severely diminished, especially mediobasal, in a case of cardiac compromise by systemic light-chain amyloidosis. The longitudinal strain in this case is reduced, especially medioapical, in an apical form of hypertrophic cardiomyopathy. Alternative methods for the assessment of longitudinal strain Feature-Traking Strain is comparable to 2D Spekle-Tracking Strain: Left ventricular mechanics assessed by two-dimensional echocardiography and cardiac magnetic resonance imaging: comparison of high-resolution speckle tracking and feature tracking, 2016 The longitudinal Unidimensional Strain (ULS) is comparable to 2D Speckle-Tracking Strain: Unidimensional Longitudinal Strain: A Simple Approach for the Assessment of Longitudinal Myocardial Deformation by Echocardiography, 2018 Longitudinal LV function may be assessed by the measurement of the anterior movement of the aortic root in systolen: Pathophysiological background and prognostic implication of systolic aortic root motion in non-ischemic dilated cardiomyopathy, 2019
|
||||||
|
Left:
a counterclockwise rotation of the apex and a clockwise rotation of the base can be determined in normal physiology.
|
|||||
©
Derliz Mereles |
||||||
|
echobasics | free echocardiography tutorial online since 2004 |
||||||

 ORC
ORC